
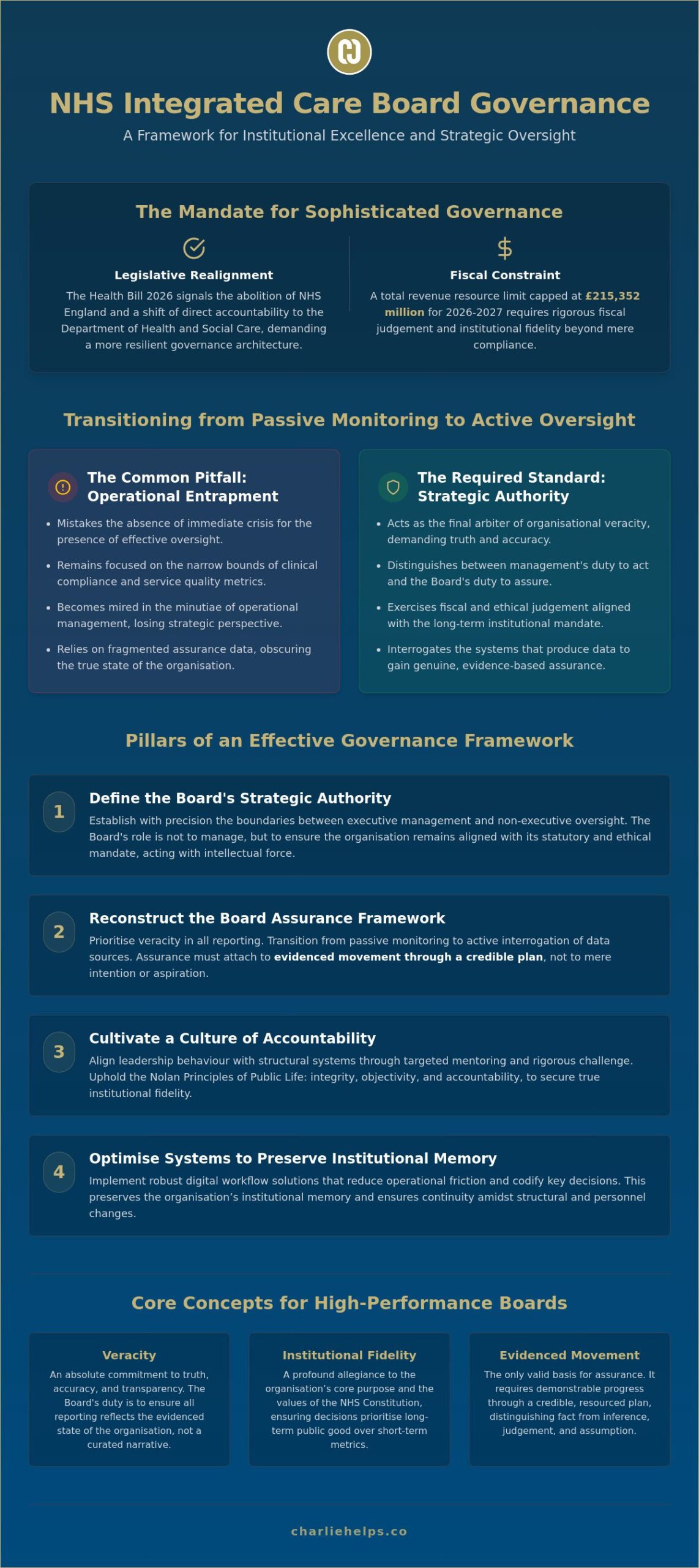
Most Integrated Care Boards mistake the absence of immediate crisis for the presence of effective oversight. This confusion often stems from a fundamental misunderstanding of the Board mandate, where directors find themselves trapped in the minutiae of operational management rather than exercising strategic authority. As the Health Bill 2026 proposes the abolition of NHS England and a shift in direct accountability to the Department of Health and Social Care, the necessity for sophisticated NHS integrated care board governance has never been more acute. Boards must now navigate a landscape where the total revenue resource limit for 2026 to 2027 is capped at £215,352 million, requiring a level of fiscal and institutional fidelity that transcends simple clinical compliance.
Directors often face the friction of fragmented assurance data across the system and the mounting regulatory pressure from the Care Quality Commission. This article provides a rigorous path toward institutional excellence, focusing on how leaders can establish veracity through evidence-based assurance and robust risk management frameworks. We will analyse the transition from passive monitoring to active, strategic oversight, ensuring your Board fulfils its statutory duties with intellectual force, practical judgement, and moral depth.
Key Takeaways
- Distinguish between clinical compliance and the overarching corporate mandate to define the strategic authority of the Board.
- Reconstruct the Board Assurance Framework to prioritise evidenced movement over mere intention, securing veracity in all regulatory reporting.
- Align leadership behaviour with structural systems through targeted mentoring to cultivate high-performance institutional fidelity.
- Optimise NHS integrated care board governance by implementing digital workflow solutions that reduce operational friction and preserve institutional memory.
- Architect a resilient governance framework to navigate the centralising legislative trends introduced by the Health Bill 2026.
The Strategic Mandate: Defining ICB Governance as an Intellectual Action
Governance is an action, not a static framework. It is a series of deliberate decisions made by directors and committees to steer an organisation toward its purpose. Within the context of NHS integrated care board governance, this mandate requires a clear distinction between clinical compliance and institutional fidelity. Whilst clinical governance focuses on patient safety and service quality, the overarching corporate mandate requires the Board to act as the final arbiter of organisational veracity. The Board must ensure that the institutional memory of the organisation remains intact, preserving the core values of the NHS Constitution amidst the structural shifts proposed by the Health Bill 2026.
The Board carries the weight of strategic authority. With the total revenue resource limit for 2026 to 2027 capped at £215,352 million, directors must exercise rigorous fiscal and ethical judgement. This is not a passive process of monitoring; it is an active exercise of power. High-performance leadership depends on the ability of the Board to see beyond the data, identifying the human behaviours and structural systems that either support or undermine the institutional mandate.
The Distinction Between Management and Oversight
The Board must define the boundaries of authority with absolute precision. Executive Directors manage operational workflows, whilst Non-Executive Directors exercise strategic oversight to ensure the organisation remains aligned with its statutory mandate. To maintain this distinction, Boards must reject consultancy theatre, the use of vague, slogan-heavy reports that obscure reality. Instead, they should foster a culture where rigorous challenge is the primary tool for achieving excellence. Reliance on evidenced movement through a credible plan is the only path to genuine assurance.
Institutional Fidelity: The Moral Depth of NHS Leadership
Institutional fidelity requires a commitment to the Nolan Principles of Public Life: integrity, objectivity, and accountability. In a complex Integrated Care System (ICS), leadership must prioritise long-term vision over short-term metrics. This moral depth ensures that the Board remains a steady hand in a complex environment, resisting the pressure of immediate crises to fulfil its foundational purpose. Clear mandates allow directors to act with intellectual force, ensuring that institutional excellence becomes a lived reality rather than a mere intention.
Risk, Assurance, and the Board’s Duty of Veracity
Veracity is the hallmark of effective NHS integrated care board governance. It represents the Board’s commitment to truth, accuracy, and transparency in all reporting. Passive monitoring of spreadsheets is insufficient; directors must instead transition to active risk oversight, where they interrogate the systems that produce data. This shift ensures the Board fulfils its duty of candour, not as a bureaucratic exercise, but as a moral imperative. When directors demand veracity, they move beyond the surface of clinical compliance to the core of institutional excellence.
A sophisticated framework integrates clinical, financial, and reputational risk into a single strategic view. The Audit Committee acts as the primary vehicle for independent assurance, providing the Board with the confidence to rely on executive accounts. To be effective, risk reporting must follow the Hemingway principle of clarity, brevity, and precision. Narrative reports should strip away the filler of consultancy theatre, focusing instead on the specific constraints, decisions, and evidence required. The King’s Fund analysis of ICSs highlights the complexity of these systems, making such clarity essential for maintaining institutional memory.
Assurance as Evidenced Movement
Assurance attaches to evidenced movement through a credible plan, rather than mere aspiration. Boards must identify the specific evidence required to support reliance on executive reports. This involves a rigorous process of distinguishing between fact, inference, and judgement. When a plan is implemented, the Board must explicitly state what risks remain and what assumptions have been made. Realising this level of precision requires a shift in leadership behaviour. Boards that struggle to bridge the gap between intention and implementation may benefit from specialist advisory support to refine their oversight mechanisms.
Veracity requires rigorous audit and internal control. Systems must be designed to expose failure rather than conceal it. By architecting governance as a series of deliberate human actions, the Board ensures that institutional fidelity remains the priority. This rigorous approach to NHS integrated care board governance protects the organisation from regulatory pressure and fosters a culture of genuine accountability. It is the Board’s duty to ensure that every report reflects the reality of the system, providing a foundation for sound decision-making and public trust.
Beyond Clinical Compliance: Cultivating a Culture of Accountability
Systems remain inert until human behaviour animates them. In the landscape of NHS integrated care board governance, structural frameworks only succeed when the individuals within them act with unwavering integrity and purpose. Systems do not fail by themselves; they fail when leadership behaviour diverges from stated institutional values. The Board must therefore set a tone that is both humane and serious, fostering an environment where accountability is a lived experience rather than a compliance requirement. This requires a shift from the passive monitoring of metrics to the active cultivation of corporate ethics.
Leadership is the engine of institutional fidelity. When directors align their actions with the Nolan Principles, they create a culture that values veracity over optics. This cultural alignment is essential for navigating the complexities of the 2026 Health Bill, which shifts accountability directly to the Department of Health and Social Care. The Board must act as the conscience of the system, ensuring that every decision is rooted in practical judgement and a clear-eyed view of the organisation’s moral mandate.
Leadership Capability and Board Dynamics
Cognitive biases often cloud strategic judgement, leading to groupthink or a false sense of security. To counter these risks, Boards must prioritise the development of their senior management teams. Many organisations utilise executive leadership coaching UK to foster strategic alignment and enhance decision-making capabilities. Professional mentoring services provide a confidential space for senior leaders to reflect on their performance, ensuring they possess the intellectual force required to lead complex systems. High-performance leadership is an architected state, realised through deliberate practice and expert guidance.
Fidelity to the Patient: The Core of NHS Accountability
The patient is the final point of accountability. Every Board decision must be weighed against its effect on patient experience, safety, and outcomes. Transparency is the bedrock of public trust; it is through transparent reporting that an organisation protects its reputation and fulfils its duty to the community. Evaluating board effectiveness requires more than a review of meeting minutes. It demands an honest assessment of how leadership actions fulfil the promise of the NHS Constitution and implement the strategic goals of the Integrated Care System. If your Board requires a partner to architect high-performance leadership, discuss our mentoring and advisory services to realise your institutional goals.
Achieving Operational Excellence through Optimised Systems
Operational excellence is the structural foundation upon which institutional fidelity is built. Without optimised systems, the reporting cycle becomes a source of friction rather than a tool for strategic oversight. Sophisticated NHS integrated care board governance requires a transition from manual data collection to automated workflows that preserve institutional memory and ensure veracity. This evolution allows directors to focus on their strategic mandate, moving beyond the administrative burden of fragmented data to exercise true authority.
Real-time strategic insights are the necessary replacement for retrospective reporting. When a Board relies on outdated information, it cannot exercise practical judgement or fulfill its duty of candour. Automated solutions provide a clear audit trail, ensuring that every decision is backed by verifiable evidence. This rigour is essential as ICBs face the performance rankings introduced by the 2026/27 NHS Oversight Framework, where scoring across seven domains requires absolute data integrity and evidenced movement.
Workflow Optimisation for the Modern Board
Bottlenecks in the production and review of board papers often obscure critical risks. Implementing workflow optimisation software allows organisations to streamline these activities while maintaining strict regulatory compliance. These SaaS solutions make governance workable in complex environments, ensuring that information flows logically from committees to the Board. Security remains paramount, particularly as the push for a single patient record increases the sensitivity of system-wide data and the need for robust digital process management.
Final Implications: The Path to Institutional Excellence
The path to excellence begins with a rigorous self-assessment of leadership capability and systemic efficiency. Conducting a board effectiveness review helps directors identify whether they are providing genuine assurance or merely reporting activity. Genuine assurance attaches to evidenced movement through a credible plan, a standard that requires both intellectual force and structural precision. For Boards seeking to realise this higher standard, partnering with corporate governance consultants UK provides the expertise required to architect a resilient future. The central question remains: does your Board have the authority, the evidence, and the systems to lead with fidelity?
Architecting the Future of Integrated Oversight
Institutional excellence is not a destination but a continuous exercise of strategic authority. To achieve this state, Boards must move beyond the theatre of clinical compliance and embrace the rigorous duty of veracity. This requires a fundamental shift in how directors perceive their mandate, treating oversight as an active, intellectual pursuit rather than a passive monitoring function. High-performance leadership depends on the alignment of human behaviour with architected systems, ensuring that every decision is backed by evidenced movement through a credible plan.
As the 2026/27 NHS Oversight Framework introduces new performance rankings, the necessity for sophisticated NHS integrated care board governance becomes a matter of institutional survival. Charlie Helps Associates provides authoritative advisory for UK public sector leaders and deep expertise in board effectiveness reviews. By utilising our proprietary Workflow Optimisation SaaS, your organisation can reduce operational friction and preserve institutional memory. We invite you to contact Charlie Helps Associates to architect your Board’s governance framework and realise a higher standard of oversight. Institutional change is possible when leadership acts with clarity, purpose, and restraint.
Frequently Asked Questions
What is the primary difference between clinical governance and corporate governance in an NHS ICB?
Clinical governance prioritises patient safety and service quality through established medical standards. In contrast, corporate governance represents the overarching strategic mandate executed by directors to ensure institutional fidelity and fiscal veracity. Whilst clinical systems monitor frontline outcomes, the Board exercises corporate authority to align the organisation with the NHS Constitution and statutory requirements.
How often should an NHS Integrated Care Board conduct a formal board effectiveness review?
Boards should conduct an internal effectiveness review annually to assess performance against strategic objectives. External reviews should occur every three years to provide independent assurance and objective scrutiny of board dynamics. Regular evaluation ensures that NHS integrated care board governance remains resilient amidst legislative shifts, such as the transition to Department of Health and Social Care oversight proposed in the 2026 Health Bill.
What are the essential components of a Board Assurance Framework for ICBs in 2026?
A robust Board Assurance Framework must include clearly defined strategic risks, identified controls, and multiple sources of assurance. It’s essential that assurance attaches to evidenced movement through a credible plan rather than mere intention. The framework should explicitly state remaining risks and the assumptions supporting board reliance on executive reports to ensure institutional veracity.
Can executive coaching improve the quality of board-level decision-making in the public sector?
Professional coaching enhances decision-making by addressing the cognitive biases that often lead to groupthink or strategic inertia. Mentoring services provide senior leaders with the intellectual force required to navigate complex systems with practical judgement. By fostering a culture of reflection, coaching ensures that leadership behaviour remains aligned with corporate ethics and the Nolan Principles.
How does workflow optimisation software reduce the burden of NHS regulatory compliance?
Workflow optimisation software reduces the administrative burden by automating the collection of assurance data and creating immutable audit trails. It eliminates the operational friction inherent in manual reporting cycles, allowing directors to focus on strategic oversight rather than data processing. These systems ensure that evidence for CQC assessments and the 2026/27 NHS Oversight Framework is readily accessible and verifiable.
What role does the ICB play in fostering a culture of accountability and candour?
The ICB sets the institutional tone by acting as the ultimate arbiter of organisational veracity and corporate ethics. Directors fulfil their duty of candour through transparent reporting and an unwavering commitment to patient outcomes. By architecting a culture where challenge is valued, the Board ensures that accountability becomes a lived experience throughout the Integrated Care System.
Disclaimer
The articles published on CharlieHelps.co are provided for general information, reflection, and commentary. They draw on professional experience, research, and interpretation, but they do not constitute legal, regulatory, financial, clinical, governance, risk, compliance, assurance, or other professional advice. Nothing published on this site should be relied upon as practice guidance, formal instruction, or a substitute for proper professional consultation. Readers should seek advice from suitably qualified advisers before acting on, applying, or relying upon any material in relation to their own organisation, Board, duties, circumstances, or decisions. Although reasonable care is taken to ensure that articles are accurate and current at the time of publication, no warranty is given as to completeness, accuracy, timeliness, or fitness for any particular purpose. Law, regulation, policy, standards, and recognised practice may change, and context matters. References to external sources, organisations, products, services, or third-party materials are included for information only. They do not imply endorsement unless expressly stated. Where an article contains affiliate links, sponsored references, or commercial relationships, these will be disclosed where relevant. The views expressed are those of the author unless otherwise stated. Reading, sharing, or responding to material on this site does not create a client, adviser, fiduciary, or professional relationship with Charlie Helps FRSA, CharlieHelps.co, or any associated entity. Readers remain responsible for their own judgement, decisions, and actions.
