
Compliance is not a surrogate for care. Whilst the pursuit of NHS Quality and Safety often dissolves into a sequence of administrative rituals, true institutional fidelity requires a more rigorous architectural approach from the Board. You likely recognise the exhaustion of regulatory fatigue, where the pressure to tick boxes obscures the primary mandate of clinical assurance. This guide offers a lucid framework for leaders to bridge the chasm between high-level data and the visceral reality of the ward.
By examining the 10-Year Quality Strategy published on 14 July 2026, we provide the intellectual tools necessary to transform oversight into verifiable movement. We will explore how directors can implement the new NHS Workforce Standards to protect staff, refine institutional memory regarding safety incidents, and satisfy the urgent requirements of Martha’s Rule. This analysis moves beyond mere intention, offering a structured path to realise a culture where safety is an active, evidenced achievement rather than a static goal.
Key Takeaways
- Boards must view NHS Quality and Safety as a deliberate expression of their authority, moving beyond the passive observation of clinical outcomes.
- Directors can utilise the Patient Safety Incident Response Framework (PSIRF) to translate raw data into verifiable assurance, ensuring that clinical reality aligns with strategic intent.
- Recognise that regulatory compliance represents the minimum threshold of operation, whilst true excellence requires the Board to architect systems that surpass mere box-ticking.
- Implement a five-step framework to transition from safety intentions to evidenced movement, supported by specific leadership capability development.
- Embed a culture of veracity by positioning board effectiveness reviews and executive coaching as the primary mechanisms for sustaining institutional memory.
The Board’s Mandate: Defining NHS Quality and Safety in 2026
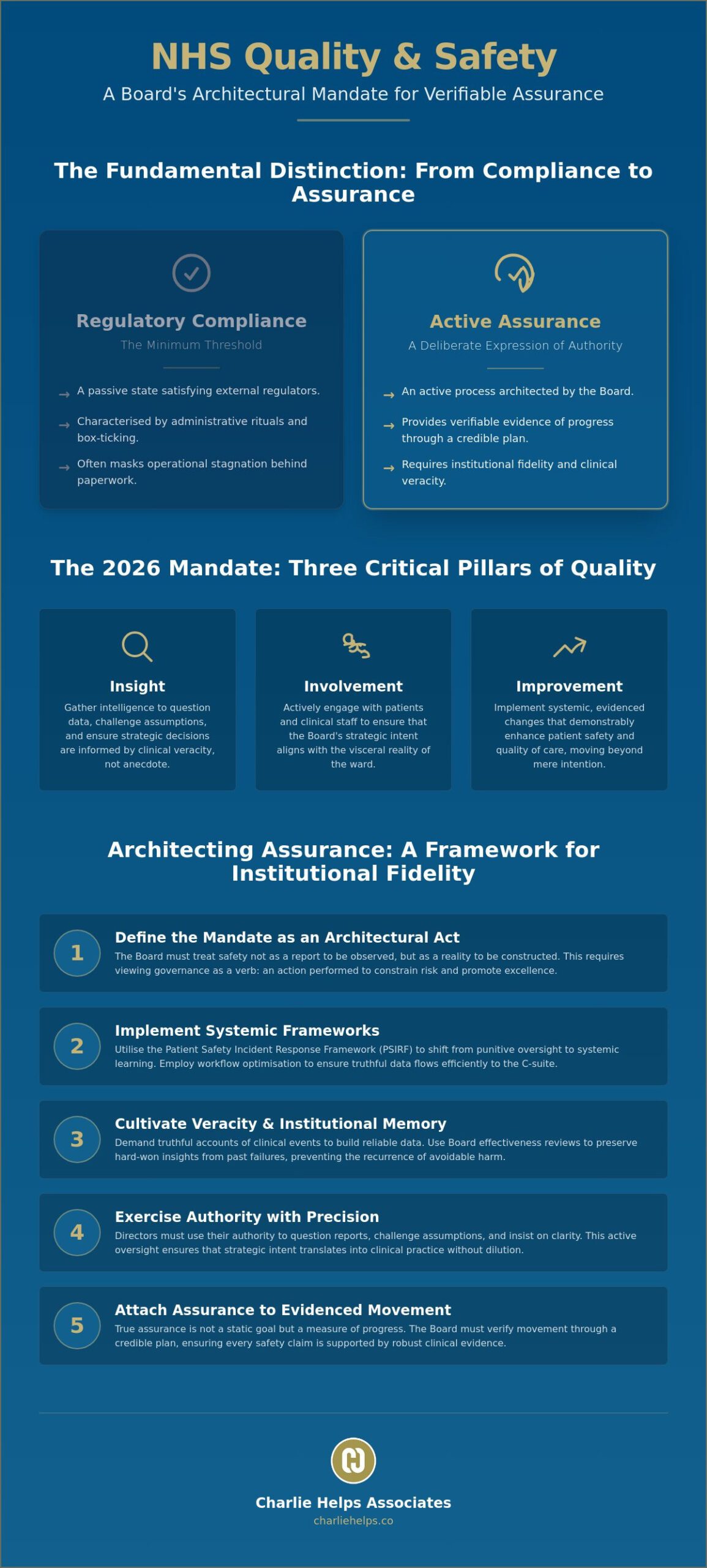
The Boardroom is the architect of clinical reality. If safety fails on the ward, the failure began at the table. NHS Quality and Safety is not a byproduct of clinical effort; it is a deliberate expression of institutional fidelity. Directors must view the quality of care as a direct result of their authority, decisions, and constraints. When a Board treats safety as an active mandate rather than a passive report, it establishes the veracity required for genuine excellence.
The 2026 landscape demands a rigorous shift in focus. NHS England’s 10-Year Quality Strategy, published on 14 July 2026, identifies three critical pillars: insight, involvement, and improvement. These are not abstract ideals; they are specific requirements for directors to gather intelligence, engage patients, and implement change. Whilst a Clinical Governance Framework provides the necessary structure, only the Board can provide the intellectual force to make it workable.
Governance as a Verb: The Role of the Director
Directors do not merely oversee safety; they act to constrain risk and promote excellence. This requires a clear mandate that permeates every level of the Trust, ensuring that strategic intent aligns with clinical practice. Individual directors exercise their authority by questioning data, challenging assumptions, and insisting on clarity. The Board’s responsibility for safety includes the active preservation of institutional memory, ensuring that the hard-won insights from previous failures dictate the constraints of current practice.
The Philosophical Shift from Compliance to Assurance
Compliance is a floor, not a ceiling. Passive compliance merely satisfies a regulator, whilst active assurance provides evidence of progress. We position this distinction as central to our role as Professional Corporate Governance Consultants UK. Assurance attaches to evidenced movement through a credible plan, whereas compliance often masks stagnation behind a veneer of paperwork. Boards must move beyond the “box-ticking” culture to achieve a state of verifiable assurance, where every safety claim is supported by robust, clinical evidence.
Architecting Assurance: The Mechanics of Institutional Fidelity
Assurance requires more than a signature on a policy document. It demands an integrated framework where the Board actively prioritises NHS Quality and Safety through structural design. Fidelity to the safety plan must supersede the allure of superficial slogans. Directors should focus on evidenced movement, ensuring that every layer of the organisation adheres to the core mandates of the NHS Patient Safety Strategy. By using insight from Learn from Patient Safety Events (LFPSE), the Board can inform strategic decisions with clinical veracity rather than anecdotal assumptions.
The Patient Safety Incident Response Framework (PSIRF)
The transition to PSIRF represents a shift from punitive oversight to systemic learning. Directors must oversee this transition with practical judgement, ensuring that the organisation focuses on why failures occur rather than who is at fault. This framework relies on veracity in incident reporting. Without honest data, the Board cannot achieve long-term safety goals. Leaders must demand truthful accounts of clinical events to preserve institutional memory and prevent the recurrence of avoidable harm.
SaaS and Workflow Optimisation in Safety Governance
Digital process management tools reduce the operational friction that often hinders safety reporting. When Boards implement a Workflow Optimisation Software solution, they create a clearer path for data to reach the C-suite. This architecture allows for the integration of AI governance, which assists directors in predicting and mitigating risks before they manifest as clinical incidents. These systems make the safety plan workable by automating routine tasks, allowing leaders to focus on high-level strategic assurance. If you require a partner to help architect these systems, you might consult our advisory team for specialist guidance.
Beyond Regulatory Compliance: Cultivating Veracity in Clinical Oversight
Governance is frequently dismissed as a bureaucratic hurdle to clinical care. This view is a category error. Effective oversight does not obstruct care; it secures it. Whilst NHS clinical governance provides the structural blueprint, directors must ensure that veracity remains the foundation of all clinical data. Regulatory compliance represents the floor of institutional operation, not the ceiling of excellence. Boards that settle for mere compliance risk a slow drift into mediocrity, where the absence of a regulatory breach is mistaken for the presence of safety.
Veracity serves as the bridge between clinical data and executive assurance. When directors demand truthful reporting, they enable the organisation to learn from its errors rather than concealing them. This commitment to truth requires a culture where staff feel safe to speak, and where the Board listens with the intent to understand rather than to blame. Credible assurance cannot exist without a foundation of honest, unvarnished data that reflects the actual clinical reality on the ward.
Martha’s Rule and the Democratisation of Safety
Martha’s Rule exemplifies the democratisation of safety. Boards hold the authority to ensure that helplines are workable and that clinical staff respect these channels without reservation. Accepting patient-led escalation requires a specific shift in human behaviour, moving away from professional defensiveness toward collaborative oversight. Martha’s Rule forces the integration of patient intuition into the Board’s risk oversight framework, ensuring that NHS Quality and Safety remains a lived reality rather than a policy ambition. It creates a feedback loop that bypasses traditional clinical hierarchies, providing directors with a direct line to the patient experience.
The Board Effectiveness Review as a Safety Tool
Evaluating how a Board functions is an essential safety action. A Board Effectiveness Review acts as a diagnostic tool to reveal hidden risks within clinical oversight. Dynamics such as groupthink or a lack of challenge can obscure systemic failures before they manifest as harm. External advisors provide the unvarnished truth necessary for the C-suite to implement meaningful change. This process ensures that the Board possesses the intellectual force required to fulfil its mandate and maintain institutional fidelity.
Realising the Safety Plan: Actionable Governance for NHS Leaders
A safety plan without evidenced movement is merely a document of intent. To achieve genuine NHS Quality and Safety, leaders must bridge the gap between strategic mandate and clinical reality. This transition requires more than just a digital strategy; it demands the implementation of systems that make safety workable on the front line. Ultimately, the safety of a patient reflects the moral depth and strategic discipline of the Board. Directors must move beyond the passive reception of reports to the active architecting of a culture that values veracity above all else.
Strategic Leadership Development and Mentoring
C-suite mentoring is essential for navigating the complexities of modern healthcare oversight. Directors often face immense regulatory pressure, requiring them to make difficult judgements where data may be incomplete or conflicting. Through Executive Leadership Coaching UK, leaders can develop the capability to maintain institutional fidelity whilst under scrutiny. This development ensures that the mandate for safety remains a lived priority rather than a secondary concern to financial or operational targets. Mentoring provides the steady hand required to lead through the noise of institutional fatigue.
A Five-Step Action Plan for NHS Boards
Moving from a safety intention to evidenced movement requires a methodical approach. Boards should adopt this five-step plan to ensure their oversight is both rigorous and effective:
- Step 1: Establishing the Aim. Clearly define the safety outcomes required and identify which individuals or committees hold the authority to achieve them.
- Step 2: Identifying Evidence. Determine what specific data and clinical indicators the Board requires to feel a sense of credible assurance.
- Step 3: Implementing Workflow Optimisation. Utilise digital tools to reduce operational friction, ensuring that safety reporting is a seamless part of clinical practice.
- Step 4: Reviewing Fidelity. Conduct regular audits of institutional memory to ensure that past lessons continue to inform current safety constraints.
- Step 5: Seeking Expert Assurance. Contact Charlie Helps Associates for a bespoke governance review to verify the effectiveness of your safety architecture.
The final test of any governance system is its utility in a crisis. Directors must decide whether their current framework provides the veracity needed to rely on clinical reports. Risks will always remain in healthcare, yet a Board that prioritises evidenced movement through a credible plan ensures those risks are known, constrained, and actively managed. True safety is not the absence of incidents, but the presence of a resilient, informed, and courageous leadership.
Architecting the Future of Clinical Assurance
The Boardroom is where safety begins. Effective oversight requires directors to move beyond the passive observation of clinical reports, opting instead for the active architecting of institutional fidelity. We have explored how the 10-Year Quality Strategy and the transition to PSIRF demand a new level of strategic discipline. These frameworks only become workable when the Board insists on veracity and preserves the institutional memory required to prevent the recurrence of harm. True NHS Quality and Safety is the result of people exercising authority with restraint, precision, and a commitment to clinical truth.
To sustain this culture, leaders must prioritise their own development through mentoring and rigorous self-assessment. Our Board Effectiveness Reviews for NHS Trusts and specialist advisory in public sector governance provide the unvarnished insights necessary to realise your strategic mandate. By aligning executive capability with clinical reality, you can transform safety from a regulatory requirement into a verifiable institutional achievement. The path to excellence is paved with evidenced movement through a credible plan.
We remain optimistic about the potential for transformation within the NHS. Through executive mentoring for clinical leaders and a steadfast focus on governance architecture, your Board can provide the steady hand needed to navigate this complex environment. We invite you to lead with purpose, ensuring that every decision serves the primary aim of patient safety.
Frequently Asked Questions
What is the Board’s primary responsibility regarding NHS Quality and Safety?
The Board holds the ultimate authority to architect a strategic mandate for NHS Quality and Safety, ensuring that clinical veracity is maintained across all services. Directors do not merely observe safety outcomes; they decide the structural constraints, resource allocations, and cultural priorities that make excellence possible. This responsibility requires moving beyond the passive receipt of reports to achieve active assurance, where every safety claim is supported by evidenced movement through a credible plan.
How does the Patient Safety Incident Response Framework (PSIRF) differ from previous models?
PSIRF shifts the organisational focus from linear investigations toward systemic learning, improvement, and cultural change. Unlike previous models that often prioritised the assignment of individual blame, this framework encourages directors to examine the underlying structural failures that lead to incidents. Boards use this framework to gather deeper insights, allowing them to implement changes that address the intersection of human behaviour and system design to prevent the recurrence of harm.
Why is institutional memory critical for maintaining safety standards in the NHS?
Institutional memory ensures that hard-won lessons from previous clinical failures continue to inform current practice, policy, and decision-making. Without this preserved knowledge, organisations risk falling into a cycle of recurring incidents as staff rotate, shift, and fade. Boards maintain this memory by embedding past insights into their risk oversight frameworks, ensuring that collective experience constrains future risks and sustains high standards of care over the long term.
Can digital workflow optimisation software improve clinical safety outcomes?
Digital workflow optimisation software reduces the operational friction that frequently hinders the timely reporting and analysis of clinical risks. By streamlining administrative processes, these tools ensure that accurate data reaches the Board with the veracity required for strategic decision-making. This architecture allows directors to respond to emerging safety concerns with practical judgement, rather than relying on the fragmented or delayed information that often characterises manual reporting systems.
How should an NHS Board respond to a negative CQC assessment of safety?
A Board must respond to a negative CQC assessment by moving immediately from a state of passive compliance to one of active, evidenced assurance. Directors should establish a credible improvement plan and provide regular evidence of movement through that plan to regulators, staff, and the public. This process often begins with a rigorous board effectiveness review to identify the oversight failures that allowed risks to manifest and remain undetected.
What role does executive coaching play in embedding a safety culture?
Executive coaching provides C-suite leaders with the intellectual force required to maintain institutional fidelity whilst navigating the complexities of healthcare oversight. It assists directors in developing the practical judgement needed to lead through regulatory pressure, institutional fatigue, and systemic change. By focusing on the human element behind the data, coaching helps leaders embed a safety culture where veracity is prioritised and the Board’s mandate is realised.
Disclaimer
The articles published on CharlieHelps.co are provided for general information, reflection, and commentary. They draw on professional experience, research, and interpretation, but they do not constitute legal, regulatory, financial, clinical, governance, risk, compliance, assurance, or other professional advice. Nothing published on this site should be relied upon as practice guidance, formal instruction, or a substitute for proper professional consultation. Readers should seek advice from suitably qualified advisers before acting on, applying, or relying upon any material in relation to their own organisation, Board, duties, circumstances, or decisions. Although reasonable care is taken to ensure that articles are accurate and current at the time of publication, no warranty is given as to completeness, accuracy, timeliness, or fitness for any particular purpose. Law, regulation, policy, standards, and recognised practice may change, and context matters. References to external sources, organisations, products, services, or third-party materials are included for information only. They do not imply endorsement unless expressly stated. Where an article contains affiliate links, sponsored references, or commercial relationships, these will be disclosed where relevant. The views expressed are those of the author unless otherwise stated. Reading, sharing, or responding to material on this site does not create a client, adviser, fiduciary, or professional relationship with Charlie Helps FRSA, CharlieHelps.co, or any associated entity. Readers remain responsible for their own judgement, decisions, and actions.
