
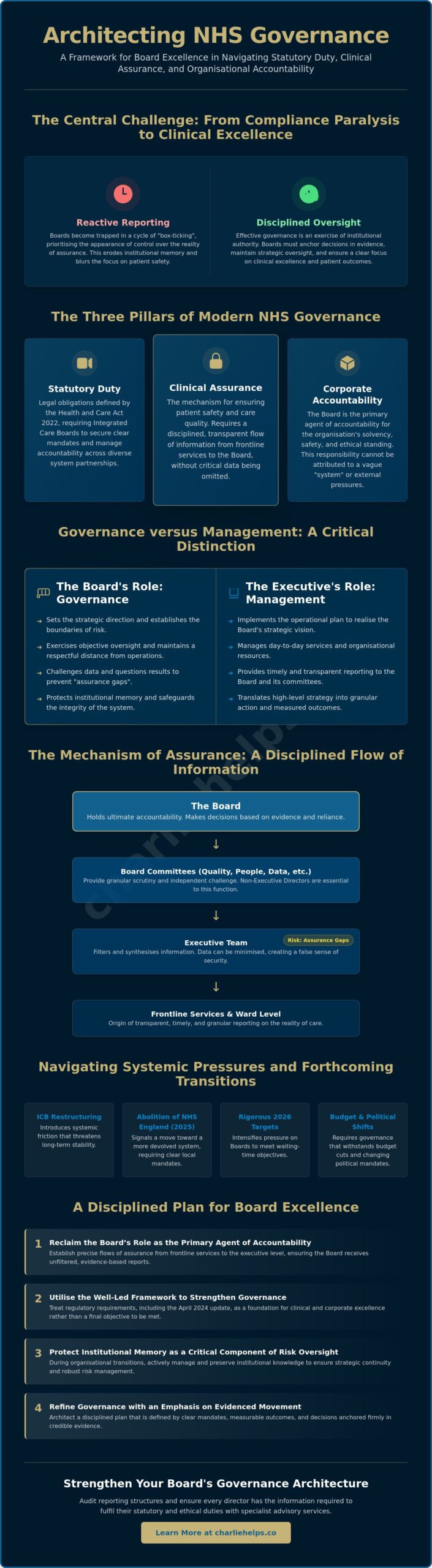
What if the perceived weight of regulatory compliance is actually the primary obstacle to the patient outcomes it intends to protect? The tension between rigid adherence to the Well-Led framework and the pursuit of clinical excellence often creates a paralysis within Integrated Care Systems. Boards frequently find themselves trapped in a cycle of reactive reporting, where the appearance of control is prioritised over the reality of assurance. Effective NHS Governance is not a performance of box-ticking; it is a disciplined exercise of institutional authority and strategic oversight. When directors fail to anchor their decisions in evidence, institutional memory erodes, and the focus on patient safety begins to blur.
You likely recognise that the restructuring of Integrated Care Boards, alongside the abolition of NHS England in 2025, has introduced a level of systemic friction that threatens to undermine long-term stability. This article provides an intellectual and practical framework to help Boards fulfil their statutory duties whilst maintaining a clear-eyed focus on organisational accountability. The following analysis explores how to architect lines of assurance that withstand the pressure of budget cuts, shifting political mandates, and the rigorous waiting-time targets set for 2026.
Key Takeaways
- Recognise how the fusion of statutory duty, clinical assurance, and corporate accountability defines the modern mandate for healthcare leadership.
- Reclaim the Board’s role as the primary agent of accountability by establishing precise flows of assurance from frontline services to the executive level.
- Utilise the Well-Led framework to strengthen NHS Governance, treating regulatory requirements as a foundation for excellence rather than a final objective.
- Protect organisational stability during transitions by treating institutional memory as a critical component of risk oversight and strategic continuity.
- Refine your governance architecture through a disciplined plan that emphasises evidenced movement, clear mandates, and measurable outcomes.
The Architecture of NHS Governance and Integrated Care
NHS Governance represents the fusion of statutory duty, clinical assurance, and corporate accountability. It serves as the structural framework that ensures healthcare organisations remain solvent, safe, and ethically sound. Historically, oversight concentrated on the individual Trust; however, the emergence of Integrated Care Systems (ICS) redirected the focus toward collaborative mandates. Boards now operate within a complex web of partnerships where authority must be explicitly defined rather than merely assumed. Directors navigate the tension between local autonomy and system-wide requirements, ensuring that the exercise of power remains rooted in evidence and ethical weight.
Statutory Duties and the Integrated Care Mandate
Boards carry legal obligations established by the Health and Care Act 2022, now further refined by the Well-Led framework updated in April 2024. Integrated Care Boards (ICBs) distribute accountability across diverse partnerships, requiring directors to manage interdependencies that extend beyond their traditional organisational boundaries. These entities must secure clear mandates before initiating large-scale changes to service models or infrastructure. Without such clarity, accountability dissipates amongst the various layers of the hierarchy, leaving the organisation vulnerable to regulatory failure. Executives must ensure that the Clinical Governance Framework remains active and rigorous across every partnership boundary, particularly as the NHS moves toward a more devolved system in 2025/26.
The Distinction Between Governance and Management
Governance is fundamentally distinct from management. The Board sets the strategic direction and establishes the boundaries of risk, whilst the executive team implements the operational plan. Maintaining a respectful distance is essential for objective oversight; it allows directors to observe the organisation with the clarity required for honest appraisal. Specific committees, such as those focused on Quality, People and Remuneration, or Data and Technology, translate high-level strategy into granular scrutiny. When directors encroach on operational agency, they risk creating shadow management structures that confuse lines of command and stifle executive initiative.
Robust oversight requires the Board to challenge data and question results without assuming the executive’s role. This discipline ensures that the Board remains a source of assurance rather than a source of operational interference. By fulfilling their oversight role, directors protect the institutional memory and safeguard the integrity of the healthcare system. The Board’s primary decision must always be whether the evidence provided supports a high level of reliance on the reported outcomes.
Board Accountability and the Mechanism of Clinical Assurance
Accountability in healthcare often dissipates within the complexities of system-wide partnerships. Boards must resist the inclination to attribute failures to a vague “system” or external pressures. The Board remains the primary agent of accountability; it holds the ultimate mandate for the safety and effectiveness of the organisation. Effective NHS Governance requires a disciplined flow of assurance that begins at the ward level and culminates in the boardroom. This reporting must be transparent, timely, and sufficiently granular to allow for meaningful intervention. When information is filtered through too many layers of management, the Board loses its ability to detect emerging risks before they manifest as harm.
Non-executive directors (NEDs) serve as the essential friction in this process. Their role is to provide independent challenge, ensuring that executive assumptions do not go unquestioned. Robust scrutiny prevents the “assurance gaps” that occur when critical data is omitted or minimised in Board reports. These gaps often hide the reality of frontline pressures, creating a false sense of security amongst leadership. Boards seeking to strengthen these internal mechanisms often benefit from specialist advisory services to audit their current reporting structures and ensure every director has the information required to act.
Defining Clinical Governance in the Modern Trust
Clinical governance is the method by which Boards fulfil their duty to protect patient interests. It synthesises clinical effectiveness, patient experience, and safety management into a single, coherent framework. The NHS Constitution establishes the foundational rights and pledges that underpin this work, providing a moral and legal compass for decision-makers. Boards realise these standards through rigorous audit and the work of specialised committees. These committees distill vast quantities of clinical data into strategic insights, allowing the Board to focus on systemic trends rather than isolated incidents.
The Role of Evidence in Board Scrutiny
Directors must distinguish between fact, inference, and management assumption. High-quality data is the only reliable basis for Board reliance. Anecdotal reports, whilst useful for context, cannot replace the rigour of quantitative evidence. Effective oversight demands a regular frequency of review, particularly when monitoring progress toward national targets, such as the March 2026 goal for 78% of A&E patients to be seen within four hours. This intellectual discipline prevents “organisational amnesia” and ensures that the Board’s decisions are rooted in the current reality of the service. Precision in evidence leads to precision in leadership.
Navigating the Well-Led Framework: Beyond Compliance
Boards frequently mistake Care Quality Commission (CQC) compliance for the ultimate measure of success. In reality, the Well-Led framework represents a baseline for safety rather than a ceiling for quality. NHS Governance reaches its full potential only when directors treat these regulatory standards as a foundation upon which to build a culture of continuous refinement. The April 2024 update to the framework introduces heightened expectations around environmental sustainability, workforce equality, and Freedom to Speak Up. Directors must analyse the eight Key Lines of Enquiry (KLOEs) not as a static checklist, but as a strategic lens through which they evaluate the health and resilience of their organisation.
Ethical behaviour cannot be mandated through policy alone; it must be lived at the highest levels of the hierarchy. When the Board models transparency and humility, these values permeate the entire workforce. A “just culture” is the prerequisite for fulfilling the statutory Duty of Candour, ensuring that when errors occur, the focus remains on learning rather than blame. This shift from retribution to restoration protects patients and staff alike, reinforcing the moral seriousness required of healthcare leaders. Boards that lead by example create an environment where staff feel safe to innovate and report risks without fear of reprisal.
The Human Element of the Well-Led Question
Board dynamics often dictate the quality of organisational oversight. Effective leadership requires more than technical expertise; it demands the emotional intelligence to navigate complex interpersonal tensions and power imbalances. Many Boards utilise Professional Corporate Governance Consultants in the UK to refine their collective decision-making through bespoke coaching and mentoring. Inclusive leadership ensures that diverse perspectives are not just present, but are actively sought to challenge groupthink. This intellectual diversity is a critical safeguard against systemic blind spots that could otherwise lead to catastrophic failures in care.
Transparency and the Duty of Candour
Openness serves as a primary defence for institutional integrity. The Board holds the ultimate responsibility for ensuring that the organisation remains candid when systemic failures occur. Transparency frameworks provide a structured method for disclosing information to patients and regulators, preventing the erosion of public trust. Within this structure, the Freedom to Speak Up Guardian acts as a vital conduit, ensuring that frontline concerns reach the boardroom directly. By supporting this role, directors demonstrate a commitment to psychological safety and operational honesty, ensuring that the Board acts on evidence rather than management assumptions.
Institutional Memory and Risk Oversight in Healthcare
Institutional memory serves as a primary bulwark against systemic failure. It represents the collective wisdom, historical context, and ethical precedents that inform current Board decisions. Within the context of NHS Governance, this memory is often the first casualty of organisational restructuring or rapid leadership turnover. When Integrated Care Boards merge or Trusts undergo transition, the resulting organisational amnesia leads to the repetition of past errors. Boards must architect deliberate systems to capture strategic insights, ensuring that the rationale behind complex decisions remains accessible to future directors.
Precision in oversight requires a long-term perspective that transcends the immediate political or financial cycle. Directors who understand the historical roots of local health inequalities or previous failed service reconfigurations are better equipped to evaluate the feasibility of new proposals. This depth of understanding allows the Board to distinguish between a genuine innovation and a recycled strategy that lacks the necessary evidence for success. Preserving this wisdom is not a clerical task; it is a strategic necessity that safeguards the organisation against the erosion of clinical and operational standards.
Succession Planning as a Governance Discipline
Succession planning remains a fundamental discipline of governance rather than a peripheral function of human resources. Directors hold the responsibility for ensuring that the organisation possesses the leadership capability to meet future challenges. Mentoring programmes provide a structured method for preserving institutional memory, allowing seasoned leaders to transfer nuanced judgment to their successors. Poor transition management in senior roles creates a vacuum of authority, increasing the risk of strategic drift and operational instability during periods of change. By treating leadership continuity as a high-level risk, the Board ensures that the organisation remains resilient regardless of individual departures.
Integrating Risk Management into Board Strategy
The Board Assurance Framework (BAF) functions as a living document of strategic intent. It allows the Board to monitor high-level risks that span multiple years, providing a longitudinal view of the organisation’s health. Directors must align their risk appetite with the pursuit of clinical excellence, ensuring that financial constraints do not compromise patient safety. In high-stakes environments, the Board may require 24/7 emergency response consulting to navigate acute crises that threaten organisational integrity. This level of oversight ensures that risk management is a dynamic behaviour rather than a static policy, allowing the Board to act with confidence when faced with unforeseen challenges.
Implementing Robust Governance: A Plan for Board Excellence
Refining the architecture of NHS Governance requires more than a passive acknowledgement of regulatory standards. It demands a methodical evaluation of how the Board exercises its authority and whether its internal structures provide genuine assurance. Directors must move beyond statements of intent, prioritising evidenced movement through a credible organisational plan. This process begins by identifying where accountability becomes diluted and where reporting structures fail to capture the reality of clinical performance. A Board that operates with intellectual rigour ensures that its oversight is both a shield for patient safety and a catalyst for organisational stability.
The Path to Governance Optimisation
Optimising the governance framework involves a series of deliberate, sequential actions. First, the Board should commission a comprehensive effectiveness review to identify assurance gaps and evaluate the quality of debate within the boardroom. This objective assessment provides the evidence required to justify structural changes. Second, directors must align the committee structure with the strategic goals of the Integrated Care System, ensuring that sub-committees have the specific mandate to scrutinise partnership-level risks. Third, the executive team should implement workflow optimisation to reduce operational friction in reporting, allowing high-quality data to reach decision-makers without unnecessary delay.
Collaborating for Excellence
Objective external appraisal often provides the clarity that internal reviews lack. Professional advisory services help Boards bridge the gap between abstract policy and daily practice, offering a steady hand during periods of systemic change. Executive coaching further enhances this process by strengthening individual director accountability and fostering a culture of professional restraint. By engaging with external mentors, Boards can refine their dynamics and ensure that every decision is rooted in a clear-eyed view of global healthcare trends. For tailored support in refining your governance architecture, you may contact Charlie Helps Associates to discuss a consultative approach to Board excellence.
The ultimate responsibility of a healthcare Board is to act with gravitas, ensuring that the organisation remains a trusted steward of public health. Directors who exercise practical judgment and maintain a respectful distance from operational management protect the integrity of the clinical mission. As the NHS moves toward the ambitious targets of 2026, the strength of its leadership will be measured by the rigour of its oversight and the clarity of its accountability. Excellence in governance is not a final destination; it is a continuous commitment to the principles of assurance, transparency, and moral seriousness.
Advancing Board Excellence in a Devolved System
The strength of a healthcare organisation resides in the clarity of its leadership and the rigour of its oversight. Directors must view NHS Governance as a dynamic discipline of assurance rather than a static obligation of compliance. By reclaiming their role as primary agents of accountability and protecting the institutional memory of their organisations, Boards ensure that clinical excellence remains a tangible reality for patients. This requires an intellectual commitment to evidence, a rejection of management assumptions, and a willingness to scrutinise the structures that support decision-making.
Achieving this level of precision often requires an objective external perspective. Charlie Helps Associates offers decades of expertise in UK public sector governance, providing the steady hand required to navigate Integrated Care System transitions. Through proprietary Workflow Optimisation SaaS for Board reporting and specialist advisory services, we help directors architect frameworks that are both resilient and lucid. Consult with Charlie Helps Associates to architect your governance framework and ensure your Board operates with the gravitas required for the challenges of 2026. Better leadership remains the most credible path toward a sustainable future for healthcare.
Frequently Asked Questions
What are the three pillars of NHS governance?
The three pillars of NHS Governance consist of clinical assurance, corporate accountability, and statutory duty. These elements ensure that the organisation remains safe for patients, financially viable, and compliant with the legal mandates established by the Health and Care Act 2022. Directors must balance these three priorities to maintain institutional integrity and protect the organisation’s clinical mission.
How does the Care Quality Commission (CQC) assess governance?
The CQC assesses governance through the Well-Led framework, which was updated in April 2024 to align with the Single Assessment Framework. Inspectors evaluate leadership dynamics, organisational culture, and the effectiveness of Board-level scrutiny across eight key lines of enquiry. They seek evidence that the Board acts on accurate data to mitigate risks and improve clinical outcomes rather than relying on management assumptions.
What is the difference between clinical and corporate governance in the NHS?
Clinical governance focuses on the systems that ensure high standards of patient care and safety, whilst corporate governance concerns the broader strategic direction, financial control, and legal compliance of the Trust. Although they overlap, corporate governance provides the structural framework within which clinical excellence is realised. The Board holds the ultimate mandate for both spheres, ensuring that financial decisions do not compromise patient safety.
Can a Board delegate its statutory duties to an Integrated Care Board?
A Board cannot delegate its core statutory duties to an Integrated Care Board, as legal accountability remains with the specific entity defined in legislation. Whilst ICBs facilitate system-wide collaboration and resource allocation, individual Boards retain the authority and the legal responsibility for their own organisation’s performance. Directors must ensure that partnership agreements do not obscure these clear lines of accountability or weaken the mechanism of assurance.
How often should an NHS Trust conduct a Board effectiveness review?
NHS Trusts typically conduct an external Board effectiveness review every three years, supplemented by annual internal self-assessments. These reviews identify assurance gaps and evaluate whether the current committee structure supports robust decision-making. Regular evaluation ensures that NHS Governance remains effective during periods of transition, providing directors with the opportunity to refine their collective judgment and leadership dynamics.
What role does institutional memory play in risk management?
Institutional memory acts as a critical safeguard by providing the historical context necessary to evaluate long-term risks. It prevents organisational amnesia, where Boards repeat past failures due to a lack of documented strategic wisdom or poor succession planning. Protecting this memory ensures that new directors make informed decisions based on evidenced historical performance, maintaining stability during mergers or leadership changes.
How can workflow optimisation software improve NHS Board assurance?
Workflow optimisation software improves assurance by streamlining the flow of data from frontline services to the boardroom. It reduces the operational friction that often leads to reporting delays or the filtering of critical information through multiple management layers. By providing a single source of truth, such tools allow the Board to act with confidence, knowing their scrutiny is based on accurate, real-time evidence rather than anecdotal reports.
Disclaimer
The articles published on CharlieHelps.co are provided for general information, reflection, and commentary. They draw on professional experience, research, and interpretation, but they do not constitute legal, regulatory, financial, clinical, governance, risk, compliance, assurance, or other professional advice.Nothing published on this site should be relied upon as practice guidance, formal instruction, or a substitute for proper professional consultation. Readers should seek advice from suitably qualified advisers before acting on, applying, or relying upon any material in relation to their own organisation, Board, duties, circumstances, or decisions.Although reasonable care is taken to ensure that articles are accurate and current at the time of publication, no warranty is given as to completeness, accuracy, timeliness, or fitness for any particular purpose. Law, regulation, policy, standards, and recognised practice may change, and context matters.References to external sources, organisations, products, services, or third-party materials are included for information only. They do not imply endorsement unless expressly stated. Where an article contains affiliate links, sponsored references, or commercial relationships, these will be disclosed where relevant.The views expressed are those of the author unless otherwise stated. Reading, sharing, or responding to material on this site does not create a client, adviser, fiduciary, or professional relationship with Charlie Helps FRSA, CharlieHelps.co, or any associated entity.Readers remain responsible for their own judgement, decisions, and actions.
