
Institutional safety is not a passive byproduct of policy; it is the result of deliberate, high-level oversight. Many directors find themselves adrift in a sea of clinical data, struggling to synthesise complex metrics into the board-level insights required for true assurance. This ambiguity regarding individual versus collective accountability often breeds a quiet fear of regulatory sanction or institutional failure. When boards treat Clinical Governance as a rigorous discipline of authority, they establish the necessary bridge between frontline practice and the boardroom mandate.
You likely recognise that mere compliance no longer suffices in a landscape where the 2026 National Model for Clinical Governance now demands consistently high-quality care. This article provides a strategic examination of clinical oversight as a framework for evidenced assurance, offering a path to improve institutional memory and manage systemic risk. We shall explore how boards move beyond abstract intentions to realise professional excellence, focusing on the outcomes-based performance of the Joint Commission’s Accreditation 360 model, and the essential role of human veracity in an era of automated clinical decision-making.
Key Takeaways
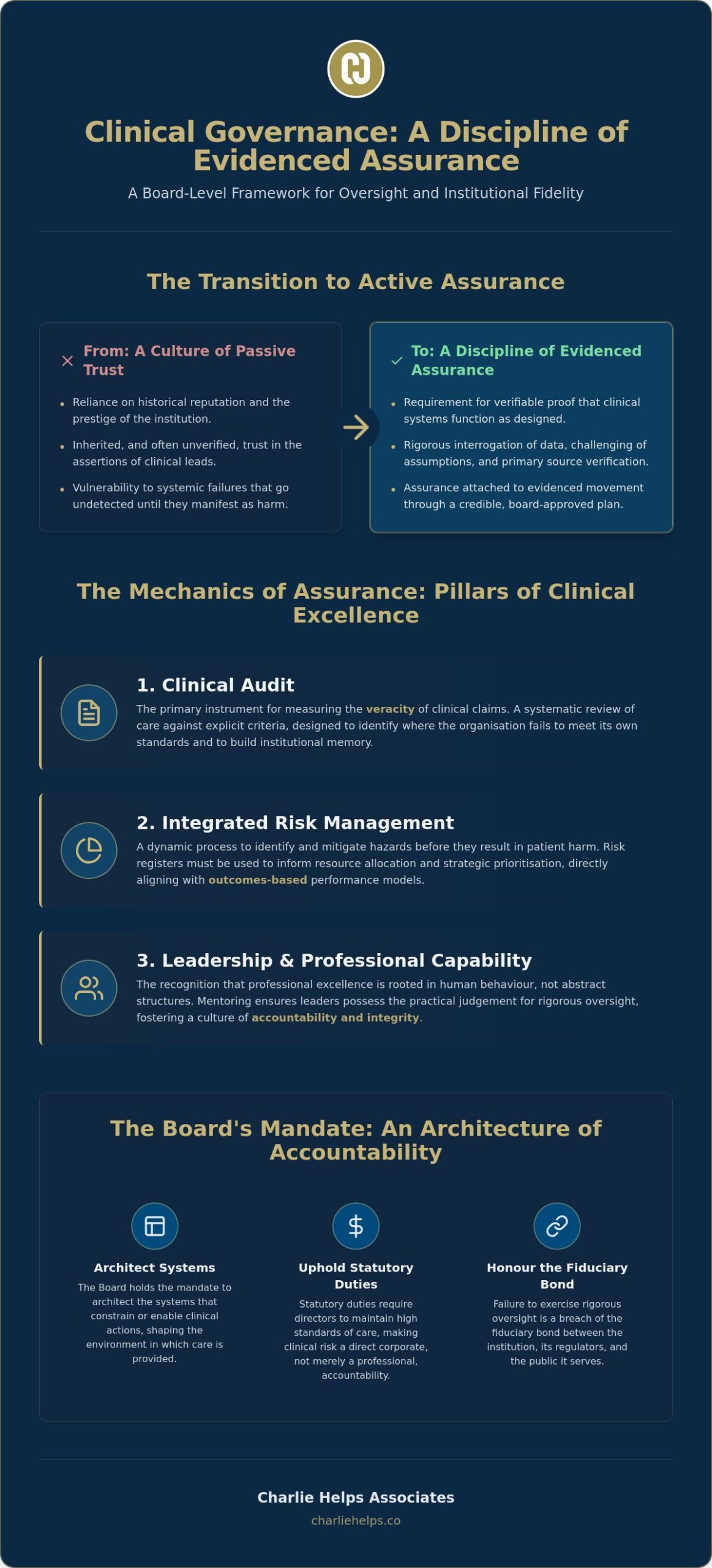
- Directors must transition from a culture of passive trust to a discipline of evidenced assurance. This shift requires the Board to verify the fidelity of clinical outcomes against professional standards.
- Boards achieve effective Clinical Governance by implementing systems of audit that establish the veracity of clinical claims. These insights allow directors to identify and mitigate hazards before they result in patient harm.
- Professional excellence is rooted in human behaviour and leadership capability rather than abstract structures. Mentoring ensures that leaders at every level possess the practical judgement necessary for rigorous oversight.
- The Board must architect a coherent governance framework that integrates clinical and corporate oversight. This integration allows leaders to synthesise data into institutional memory and informed decision-making.
The Mandate of Fidelity: Defining Clinical Governance
Clinical Governance is not a static framework or an abstract container; it is the active exercise of authority by boards and committees to ensure institutional fidelity. It represents the specific system through which directors remain accountable for the quality of services and the veracity of clinical outcomes. By treating Clinical Governance as a verb, leaders transform oversight from a bureaucratic requirement into a rigorous board-level discipline. This discipline requires directors to interrogate data, challenge assumptions, and verify that the organisation fulfils its promise of safety to every patient.
Institutional fidelity requires a moral and professional contract between the board and the public. When a board authorises a clinical strategy, it pledges that the care provided will meet established standards of excellence. To honour this contract, directors must move beyond a culture of inherited trust to one of evidenced assurance. This shift ensures that the organisation does not merely intend to be safe, but possesses the verifiable proof that its systems function as designed.
The Shift from Passive Oversight to Active Assurance
Directors often rely on the historical reputation of their clinical leads or the prestige of their institution. This passive reliance creates a vulnerability where systemic failures go undetected until they manifest as harm. The 2026 National Model for Clinical Governance, published in June 2026, marks a definitive turn toward objective data and practical application. Assurance now attaches to evidenced movement through a credible plan, rather than mere intention. Boards set the standard for clinical excellence by requiring that every claim of safety is backed by primary source verification and rigorous audit.
Statutory Duties and Board Accountability
Legal obligations for directors in the United Kingdom extend far beyond financial stewardship. Statutory duties require board members to maintain high standards of care, making clinical risk a matter of direct corporate accountability. Failure to oversee the clinical dimension of an organisation invites regulatory sanction and erodes institutional memory. Whilst individual clinicians carry professional responsibility for their actions, the Board holds the mandate to architect the systems that constrain or enable those actions. Neglecting this duty is not merely a management oversight; it is a breach of the fiduciary bond between the institution and those it serves.
The Mechanics of Assurance: Pillars of Clinical Excellence
Assurance requires a rigorous mechanism to verify that institutional intentions align with frontline reality. Clinical audit, risk management, and information management provide the board with the clarity required to exercise effective oversight. These pillars function as the sensory organs of the board, allowing directors to perceive the true state of care. A framework for healthcare organisations ensures that these mechanisms are not siloed but integrated into the central strategy of the institution.
Clinical Audit as a Tool for Institutional Memory
Clinical audit serves as the primary instrument for measuring the veracity of clinical claims. It is a systematic review of care against explicit criteria, designed to identify where the organisation fails to meet its own standards. By conducting these reviews, the Board builds institutional memory, ensuring that past errors inform future safeguards. Closing the loop is essential; an audit that identifies a flaw without a subsequent plan to rectify it is merely a record of failure rather than an active exercise of Clinical Governance. Directors must demand evidence that improvements have been realised and sustained over time.
Integrating Risk Management with Board Strategy
Effective risk management identifies and mitigates hazards before they manifest as patient harm. Boards should utilise risk registers not as static lists, but as dynamic tools to inform resource allocation and strategic prioritisation. Beginning 1 January 2026, the Joint Commission will implement its Accreditation 360 model, which emphasises outcomes-based performance. This shift requires boards to align their risk frameworks with measurable results rather than procedural compliance. Such a proactive stance ensures institutional resilience, allowing the organisation to absorb shocks whilst maintaining fidelity to its safety mandate.
Evidence-Based Practice and Clinical Fidelity
Clinical effectiveness ensures that clinicians provide care based on the best available evidence. The Board must grant staff the authority and resources to implement these best practices, reducing the variance that leads to poor outcomes. Utilising a Workflow Optimisation SaaS solution can significantly reduce operational friction, allowing professional judgement to remain the focus of clinical work. When directors ensure that practice aligns with proven medical standards, they fulfil the institutional promise of excellence. Fidelity to these standards is not optional; it is the foundation of professional accountability.
The Human Dimension: Leadership and Professional Capability
Excellence in care is not a byproduct of structural systems. It is a manifestation of human behaviour. Whilst frameworks provide necessary boundaries, the actual exercise of Clinical Governance depends upon the authority, mandate, and practical judgement of individuals. Boards must move beyond a preoccupation with process to focus on the cultivation of leadership capability at every level. This human-centric approach ensures that the organisation’s safety mandate is not just a policy document, but a lived reality.
Developing High Performance Leadership Capability
Executive leadership coaching serves as a critical tool for aligning board members with clinical objectives. By engaging in professional mentoring, directors develop the intellectual force required to interrogate complex data and challenge institutional inertia. This capability is not innate; it must be nurtured through a deliberate process of reflection and growth. Such investment ensures that those with authority possess the necessary skills to maintain institutional fidelity, even during periods of significant organisational change.
Fostering a Culture of Accountability and Learning
A culture of transparency is the only effective antidote to institutional failure. Directors must actively discourage a blame-centric environment, as fear invariably leads to the suppression of critical safety information. Instead, the Board must foster a learning culture where staff feel secure in reporting incidents and identifying systemic weaknesses. This transition requires board members to model the very behaviours they expect from the frontline, demonstrating that accountability is about collective improvement rather than individual punishment.
Succession Planning and Institutional Memory
Institutional memory is often the first casualty of leadership turnover. To safeguard clinical standards over time, boards must implement rigorous succession planning and mentoring programmes. These initiatives ensure that the wisdom gained from past challenges is transferred to the next generation of leaders. By prioritising the long-term development of clinical leadership, the Board protects the institution against the risks of cultural drift and professional stagnation. If you require expert guidance in architecting these leadership frameworks, our advisory and coaching services provide the steady hand necessary for success.
Architecting the Path to Operational Excellence
Boards must implement a clear governance architecture that integrates clinical and corporate oversight. This integration prevents the formation of clinical silos, which often obscure systemic risks from the boardroom. Assurance is not a feeling of comfort; it is achieved through the rigorous application of data and professional judgement. When directors align clinical activity with institutional purpose, they ensure that the organisation remains faithful to its strategic mandate.
Integrating Governance Frameworks for Strategic Value
An integrated governance framework treats clinical outcomes as a primary indicator of organisational health, rather than a secondary concern for medical staff. By architecting these systems, boards improve performance and reduce the friction between corporate and clinical objectives. Corporate governance consultants provide the expertise necessary to design these structures, ensuring that every committee has a clear mandate and defined authority. This alignment allows the board to see the organisation as a single, coherent entity, rather than a collection of disparate departments.
Decision-Making and Risk Accountability
Every board-level decision requires three components: evidence, authority, and a thorough risk assessment. Directors must evaluate the veracity of the information presented to them, questioning the assumptions behind the metrics. This scrutiny is essential for effective Clinical Governance. The Board carries the responsibility for ensuring that resources are allocated to mitigate high-priority risks, moving beyond mere intention to realise workable solutions. Practical judgement dictates that assurance only exists when movement through a credible plan is evidenced.
Achieving Sustainable Clinical Excellence
Success is the sustained fulfilment of the organisation’s clinical mandate. It requires a move from basic compliance to a deep-rooted culture of institutional fidelity. Regular board evaluation services ensure that the oversight mechanisms remain effective, and that directors possess the capability to meet evolving challenges. The path forward is clear: boards must act with authority, decide with evidence, and lead with purpose. To begin this transformation, you may organise a board effectiveness review with Charlie Helps Associates.
Securing Institutional Fidelity Through Active Oversight
Active oversight is the only credible path to institutional safety. By treating Clinical Governance as a rigorous board-level discipline, directors move beyond the passivity of inherited trust to the certainty of evidenced assurance. This transition requires a clear-eyed interrogation of clinical data, the implementation of integrated frameworks, and a steadfast commitment to professional standards. When boards architect these systems with precision, they ensure that the organisation’s mandate for excellence remains a lived reality rather than an abstract ambition.
True assurance is ultimately a product of human veracity and leadership capability. Our team at Charlie Helps Associates specialises in architecting institutional fidelity, providing a measured, reflective approach to strategic advisory that addresses the complexities of modern oversight. Through our expert board-level mentoring services, we support leaders in developing the practical judgement necessary to navigate clinical risks with confidence. You don’t need to navigate these systemic complexities alone.
The path to excellence is methodical and deliberate. You possess the authority to redefine your organisation’s future and to realise a culture where safety is verified through action. We invite you to contact Charlie Helps Associates to architect your governance framework and begin this essential work today.
Frequently Asked Questions
Is clinical governance a statutory requirement for all healthcare organisations in the UK?
Boards must fulfil statutory obligations for NHS trusts and private providers regulated by the Care Quality Commission. Directors carry a legal mandate to ensure the safety and quality of care under the Health and Social Care Act 2008. Failure to maintain these standards exposes the Board to regulatory intervention, potential prosecution, and a loss of public trust. This mandate requires an active exercise of authority rather than passive compliance.
Can clinical governance be integrated with corporate governance frameworks?
Boards should integrate clinical and corporate frameworks to ensure a unified view of institutional risk. Treating Clinical Governance as an isolated silo prevents directors from understanding how financial or operational decisions influence patient safety. An integrated architecture allows for the synthesis of disparate data into a coherent strategic narrative. This alignment ensures that every decision-maker understands the clinical implications of corporate strategy and resource allocation.
How much authority should the Board have over clinical decision-making?
The Board holds ultimate authority over the systems and standards of care, though it does not override individual professional judgement in specific clinical cases. Directors must set the mandate for excellence and ensure that clinicians possess the resources to fulfil it. Their role is to interrogate the veracity of clinical claims and provide the necessary constraints to ensure institutional fidelity to safety. Authority attaches to the oversight of the system, not the individual treatment plan.
What happens if a clinical governance framework fails to identify a significant risk?
When a system fails to identify a significant risk, the Board remains collectively accountable for the resulting outcome. Such failures often indicate a breakdown in institutional memory or a culture that suppresses inconvenient truths. Directors must immediately implement an emergency response and conduct a rigorous audit to identify the systemic cause. This process ensures that the organisation learns from the failure and strengthens its oversight to prevent recurrence.
What evidence supports the Board’s reliance on clinical performance data?
Boards rely on evidenced movement through a credible plan to ensure effective Clinical Governance, supported by primary source verification and independent audits. Reliance is only justified when the data demonstrates a consistent alignment with professional standards over time. Directors must verify that the information presented to them reflects the actual state of care. This interrogation of data ensures that the Board acts upon a foundation of truth rather than assumption.
What are the primary risks that remain even with a rigorous governance framework in place?
Risks associated with human behaviour and unpredictable systemic shocks remain even with rigorous oversight. Cultural drift can erode standards over time if leadership capability is not actively nurtured through mentoring and coaching. Boards must accept that no framework can eliminate all hazards. This reality necessitates a constant state of vigilance, a focus on institutional resilience, and a commitment to the perpetual improvement of safety systems.
Disclaimer
The articles published on CharlieHelps.co are provided for general information, reflection, and commentary. They draw on professional experience, research, and interpretation, but they do not constitute legal, regulatory, financial, clinical, governance, risk, compliance, assurance, or other professional advice.Nothing published on this site should be relied upon as practice guidance, formal instruction, or a substitute for proper professional consultation. Readers should seek advice from suitably qualified advisers before acting on, applying, or relying upon any material in relation to their own organisation, Board, duties, circumstances, or decisions.Although reasonable care is taken to ensure that articles are accurate and current at the time of publication, no warranty is given as to completeness, accuracy, timeliness, or fitness for any particular purpose. Law, regulation, policy, standards, and recognised practice may change, and context matters.References to external sources, organisations, products, services, or third-party materials are included for information only. They do not imply endorsement unless expressly stated. Where an article contains affiliate links, sponsored references, or commercial relationships, these will be disclosed where relevant.The views expressed are those of the author unless otherwise stated. Reading, sharing, or responding to material on this site does not create a client, adviser, fiduciary, or professional relationship with Charlie Helps FRSA, CharlieHelps.co, or any associated entity.Readers remain responsible for their own judgement, decisions, and actions.
